Piriformis syndrome no longer exists
You might recognise it. A nagging, sometimes more shooting pain that starts in the buttock and slowly finds its way to your leg. Maybe for a few weeks now. Maybe for longer. You've tried to ignore it, started moving more carefully but the symptoms won't subside. These symptoms are relatively common and we usually refer to it as piriformis syndrome. But what if we told you that this diagnosis is more complicated than we previously thought? And that the most common treatment, stretching the piriformis, often does more harm than good in cases of genuine irritation of the nerve? High time to take a closer look at this issue.

A diagnosis with an expiry date: the history of piriformis syndrome
In 1947, Dr Robinson first described the term “piriformis syndrome” as an explanation for pain in the buttock radiating along the sciatic nerve. It was an era when imaging was in its infancy and good clinical reasoning clearly had its limits. A simple anatomical explanation was a logical way to explain symptoms.
For a very long time, piriformis syndrome became the standard diagnosis for almost any kind of buttock pain with radiation. In this way, complaints in the buttock with radiation were diagnosed for almost seventy years. An impressive time for a diagnosis that has much more depth than we thought.
In 2015, the term was officially replaced. By a new description namely: Deep Gluteal Syndrome, abbreviated DGS (Martin et al., 2015). Not because complaints around the piriformis do not exist, but because the name piriformis syndrome is too simple and one-sided an explanation for something that is anatomically much more complex. Officially, DGS is seen as pain in the buttock region caused by a non-discogenic(intervertebral disc, i.e. spinal) entrapment of the sciatic nerve.
The piriformis is not the only suspect
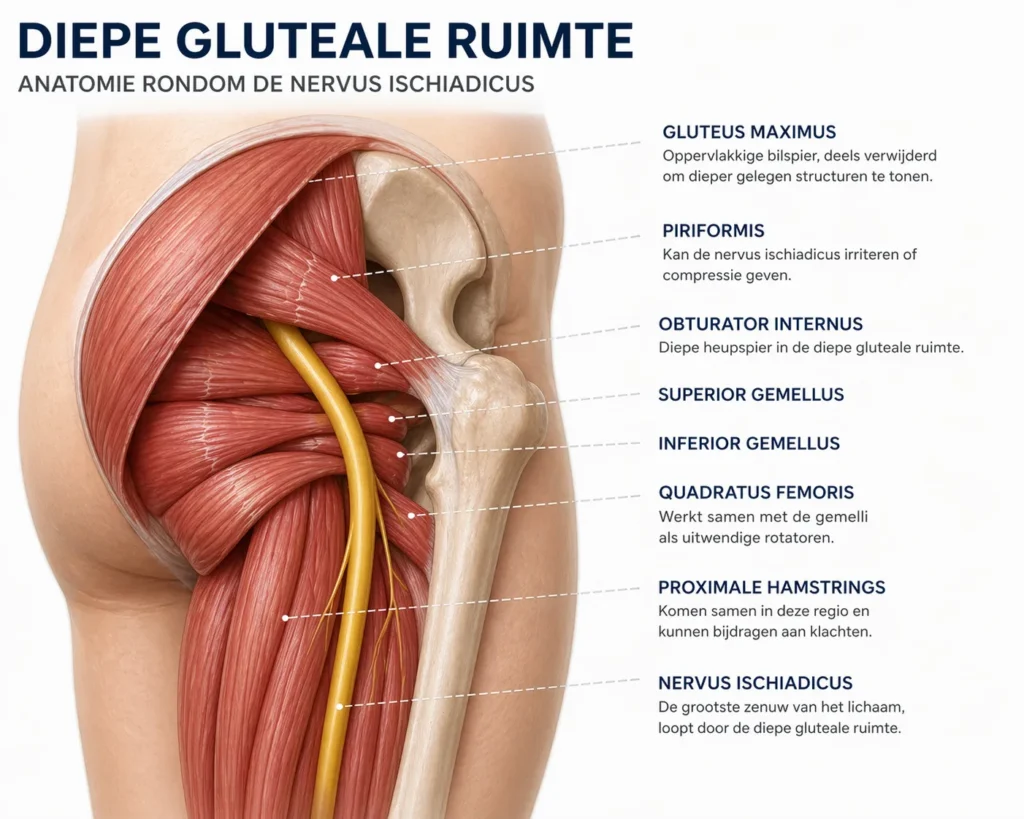
To understand why this name change is so important, we need to reflect on what goes on in the deep gluteal space. This is the anatomical region deep in the buttock, where the sciatic nerve(large nerve) has to find its way through an area full of different structures.
The deep gluteal space does not consist only of the piriformis. Other muscles such as the obturator internus, the gemelli, the quadratus femoris and the proximal hamstrings can also exert pressure on the sciatic nerve. In addition, fibrovascular ligaments, scar tissue, vascular abnormalities and in rare cases, space-occupying tissues such as cysts or tumours can excite the nerve.
And in particular, fibrovascular ligaments often seem to cause symptoms. These connective tissue structures can be found endoscopically in about 40% of patients with DGS, but what is interesting, these structures are not visible on a standard MRI.
An unequivocal answer to the question of which structure causes pressure on the nerve is very difficult to answer.
Added to this, in about 16% of people, the sciatic nerve does not pass under the piriformis, but through it or just above it (Smoll et al., 2010). In this group, the piriformis may not anatomically be the direct cause at all. Major MRI examination (Bartret et al., 2018) also confirms this. In 1039 individuals, although some 20% found anatomical variants of the sciatic nerve, there was no correlation between those variants and the occurrence of symptoms.
How common is it?
Of all patients who actually suffer from sciatica, only 8% actually have piriformis syndrome (Stafford et al., 2007). Broader view: of all people who present with back pain and radiation in the leg, about 20% eventually turn out to have Deep Gluteal Syndrome (Hopayian & Heathcote, 2019). The vast majority of people with buttock pain and radiation have another cause, such as nerve root compression due to a herniated disc or stenosis.
How do you recognise it? The clinical picture
Common complaints in DGS are pain in the buttock or hip, tenderness in the buttock region and pain radiating down the back of the leg. The pain is often unilateral and increases when bending the hip combined with knee extension. We also see that people have difficulty sitting for long periods, sometimes have a different walking pattern, have decreased sensation in the leg and often experience more symptoms at night, which seem to be milder during the day.
The piriformis stretch problem: when an exercise backfires
This is where it gets interesting and surprising for many patients and therapists. The piriformis stretch is probably the most commonly prescribed exercise for buttock pain with radiation. It feels familiar, logical and, for many people, even relieving. But there is a mechanism behind it that deserves attention.
During hip flexion, the movement that includes stretching the piriformis. The nerve moves, slides and stretches with the movement (Coppieters et al., 2006). In a completely healthy nerve, the connective tissue surrounding the nerve has enough room to accommodate this. But with local irritation, the nerve tissue becomes hypersensitive, not only to pressure but also to movement and stretch (Wall, 1992). What experience does tell us is that some patients with nerve-related buttock pain respond poorly to stretching the buttock(Martin et al., 2015). The paradoxical effect is that muscle stretching feels like relief, but at the same time the already irritated nerve may be repeatedly stimulated. The relief is temporary and superficial. This is what we call a maladaptive effect, you keep stretching because it seems to help, but in fact it maintains the irritation or worsens the situation.
How to determine DGS correctly?
If an MRI is not enough and “piriformis syndrome” says too little, how do you arrive at the right diagnosis and more importantly approach? The answer lies in an approach that combines three components.
Physical testing: No test stands strong on its own. But the combination of the Seated Piriformis Stretch Test and the Active Piriformis Test still performs remarkably well. Together, they give a sensitivity of 91% and a specificity of 80% (Martin et al., 2015).
Briefly:
When both tests show no symptoms, the chances of someone having DGS anyway are slim. So you can be reasonably confident that it is not present. You don't 100% rule it out, but it's a lot less likely.
When both tests show symptoms, there is a strong indication that deep gluteal syndrome is indeed present. However, not everyone with two positive tests actually has it. 1 in 5 people do not have it but still score positive.
Other tests described are the Freiberg Sign, the FAIR test, the Beatty Manoeuvre and the heel-contralateral knee manoeuvre, but diagnostic accuracy studies are lacking for these tests.
Targeted palpation also helps determine which structure may be involved, but for treatment in first-line settings, that distinction still makes no difference in most cases.
MRI remains valuable to rule out serious pathology such as tumours or large tendon tears. But a normal result does not mean nothing is wrong. The most common causes of DGS, such as fibrovascular bands, are only visible endoscopically and do not remain visible on a standard MRI. Therefore, when symptoms remain but the MRI shows nothing, it does not mean that DGS cannot be present.
What can you do about it? Treatment
In the short term, the most important thing is to reduce activities that aggravate pain. Avoid sitting or standing for long periods and change positions as often as possible. The human body simply does not like static positions. Sitting on a good cushion can make sitting more bearable. A pillow between the legs in bed can reduce prolonged stretching of the glutes. If running or walking is painful, reduce it temporarily to an acceptable level. Other short-term options include manual therapy, massage in the painful area and some people respond well to dry needling.
In the long term, a structured exercise programme targeting the painful area is effective. Make sure the pain is tolerable during the programme and that any increased pain afterwards disappears within 24 to 48 hours. If not, simplify the exercises or reduce the number of sets and repetitions.

Other thoughts on buttock pain with radiation
Deep gluteal syndrome is not something new and not just a new name for the same symptoms. It is an educated adjustment to an overly narrow view of a complex anatomical area. The deep gluteal area is not a one man show. The sciatic nerve is not exclusively pinched by the piriformis, and a simple piriformis stretch does not automatically fix what goes wrong.
We may stop calling everything “piriformis syndrome”. And we should certainly stop reflexively prescribing piriformis stretches as the first treatment for nerve pain. A normal MRI is not definitive proof of no pressure on the sciatic nerve.
For people with complaints, the message is simpler but no less important: if you have been walking around with a diagnosis of “piriformis syndrome” for a long time and treatment is not working, it is worth having someone with a fresh pair of eyes once again. Your symptoms deserve a diagnosis that is right.
Frequently asked questions
Does piriformis syndrome exist? The symptoms are real, but the name is outdated. In 2015, “piriformis syndrome” was officially replaced by Deep Gluteal Syndrome, because the piriformis is just one of many structures that can excite the sciatic nerve.
What is the difference between Deep Gluteal Syndrome and sciatica? Sciatica is an umbrella term for anything that produces radiation along the sciatic nerve .It is not a diagnosis in itself. Deep Gluteal Syndrome is one of the possible causes, along with a herniated disc, stenosis or other conditions. About 20% of people with a sciatica diagnosis actually have DGS.
Is piriformis stretching dangerous? Not necessarily, but in an irritated sciatic nerve, aggressive stretching may actually increase nerve irritation rather than decrease it. Whether stretching makes sense depends very much on the individual situation. Have this assessed by a specialised physiotherapist.
Does a normal MRI rule out Deep Gluteal Syndrome? No. The most common causes, such as fibrovascular bands, are only visible through keyhole surgery. A normal scan explicitly does not rule out DGS. By the way, this does not mean that you need surgery right away.
Which tests are reliable? The combination of the Seated Piriformis Stretch Test and the Active Piriformis Test gives a sensitivity of 91% and specificity of 80% (Martin et al., 2015). Additional palpation helps to identify the affected structure even more precisely.

Related complaints