Upper leg injury, all about the rectus femoris
Muscle injuries account for a large proportion of all sports-related injuries. And especially in explosive sports like football and athletics. We know that 30% of injuries in football players involve muscle injuries and almost 80% of these occur in the upper leg. Of these complaints, about 20% are muscle injuries of the quadriceps. The rectus femoris is from the quadriceps group by far the most often involved, this is mainly due to its unique function in sprinting, kicking and while changing direction.
The rectus femoris is a bi-articular muscle that runs across both the hip and knee joints. This function makes it more vulnerable to so-called stretch-type injuries, where the muscle comes under tension in an extended position. In some cases, these injuries cause long-term symptoms and require careful diagnosis, treatment and rehabilitation. And a good understanding of anatomy is very important in this regard.
Anatomy of the rectus femoris
To properly place new insights, it is important to know where we are coming from. The anatomy of the rectus femoris and its associated image were first described in more detail in 1995. Thereafter, little has appeared for an extended period of time that has changed our understanding of this anatomical region. The rectus femoris belongs to the quadriceps and is distinguished by the fact that this muscle runs across two joints. Biomechanically, the muscle functions as both hip flexor and knee extensor. The rectus femoris is largely composed of type II muscle fibres. These fibres deliver short, powerful contractions as needed in sprinting, jumping and explosive changes of direction.
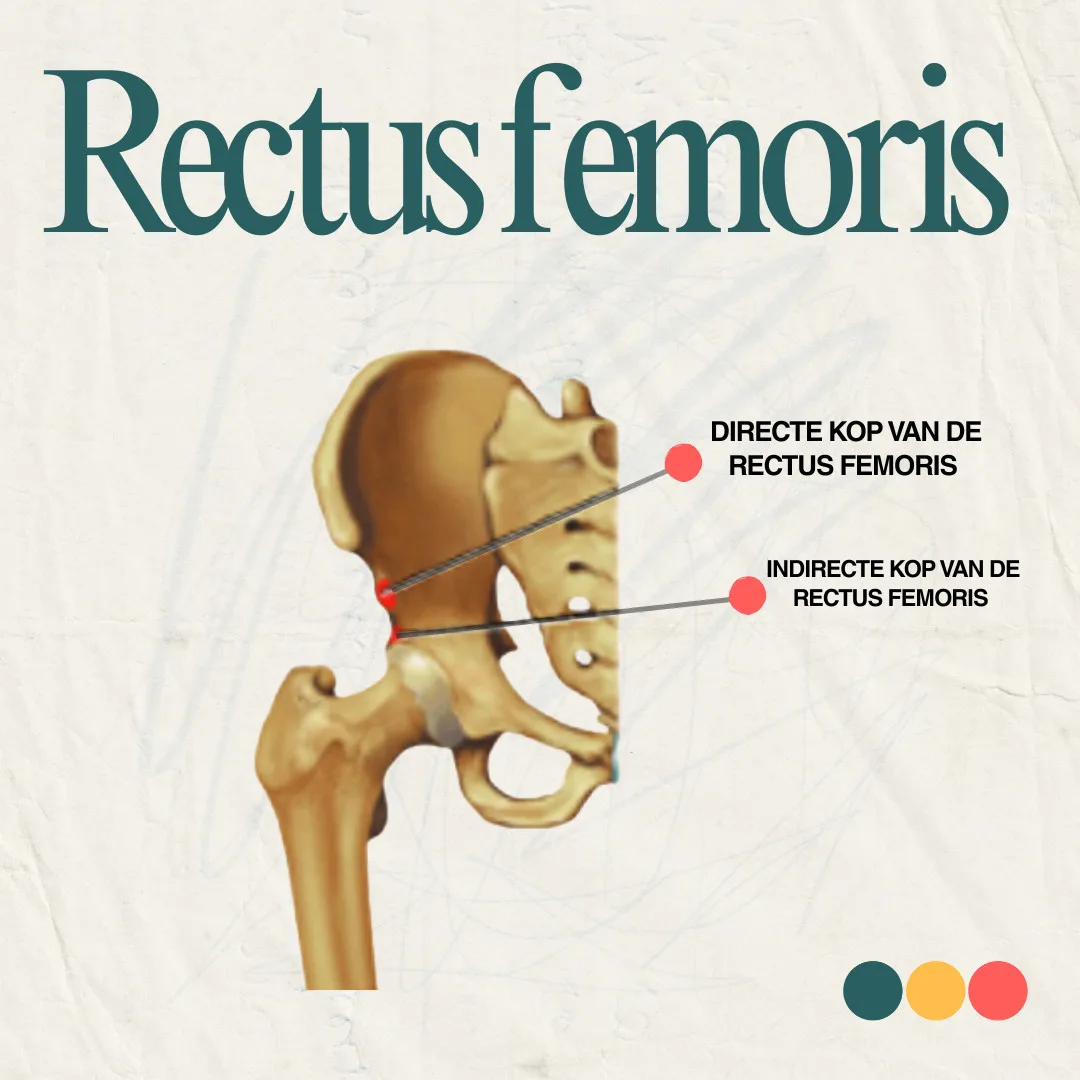
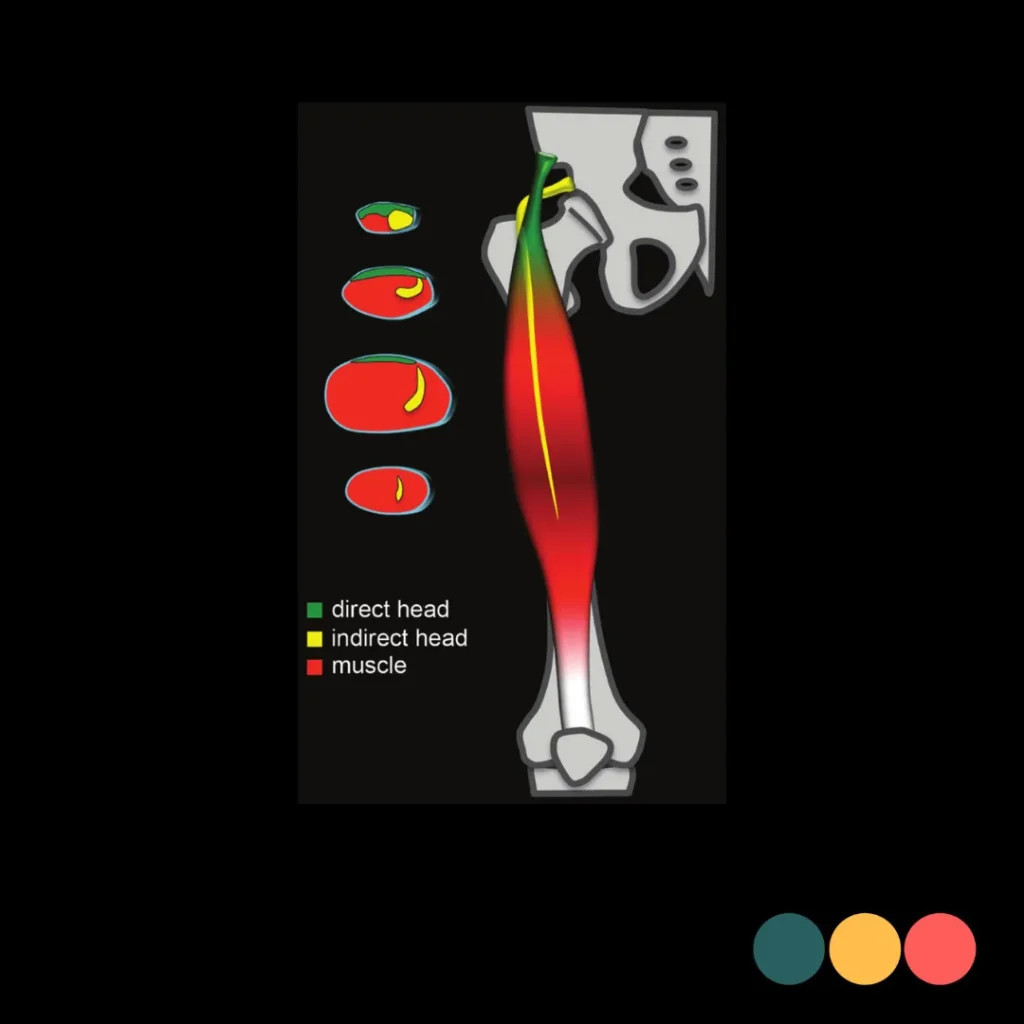
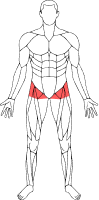
The rectus femoris has two main attachments on the pelvis: the direct head and the indirect head. Both structures have their own attachment, fibre sequence and clinical importance.
The footprint of the immediate head - the attachment surface on the spina iliaca anterior inferior (SIAI) - has an average size of 1.3 by 2.6 cm. After a few centimetres, the immediate head fuses with the joint tendon, but the muscle fibres remain largely on the outside of the muscle, continuing into the anterior tendon plate (aponeurosis). This superficial location, combined with better blood flow and less mechanical stress during explosive movements, means that injuries to this part of the muscle are usually less severe. Recovery is usually faster, with relatively short rehabilitation and a lower risk of complications. This contrasts with injuries to the central tendon, which are deeper in the muscle, have poorer blood flow and are more heavily loaded during activities such as sprinting or shooting. As also described by Kassarjian et al. (2014), the clinical outlook in injuries to the immediate head is generally more favourable.
The indirect head attaches deeper, at the level of the upper edge of the acetabulum and anterior hip capsule. This attachment is not only more complex in structure, but also has a larger footprint: on average about 1.7 by 4.7 cm, as described by Gyftopoulos et al. (2008). The fibres of this indirect head form the deep layer of the common tendon (conjoined tendon), where they meet the fibres of the direct head. From this joint structure, the central tendon develops, continuing into the muscle belly of the rectus femoris. Because this part lies deeper, is less well supplied with blood and is heavily loaded during explosive movements, injuries to this structure are often more severe. They are associated with a longer recovery time, a higher risk of scarring and an increased risk of recurrence. This is precisely why it is important to distinguish between superficial and deep injuries in both imaging and physical examination - with specific attention to the difference between the direct and indirect head.
Briefly:
Direct head, superficial fibres, faster recovery from injury.
Indirect head, central tendon, longer and more complex recovery from injury.
Capsular head, more headaches than thought?
Since 2004, our understanding of the anatomy of the rectus femoris has continued to deepen. In anatomical studies is a third tendon structure described namely the capsular head. So in addition to the direct and indirect head, there is another capsular head. This structure is not an addition to the indirect tendon, but a separate and independent part of the tendon. This tendon structure originates in the anterior hip capsule near and possibly intertwined with the ligamentum iliofemoral. This capsular head runs distally and laterally, at an angle of about 60 degrees to the immediate head, and eventually joins the joint tendon. This variant was found in about 83% of the individuals studied and mostly bilaterally(both sides). Although the exact function is still under discussion, we believe that this structure may play a role in injury patterns that cannot be well explained from the classical biceps model.
On MRI, the capsular head is difficult to see under normal conditions because of its small size and location. Only when injury occurs do the contours become more visible. This phenomenon, in which small ligamentous structures become more visible with trauma, is also known from other areas such as in the anterolateral ligament (ALL) of the knee.
The anterolateral ligament (ALL) is a small ligament on the outside of the knee. It plays along with the anterior cruciate ligament (VKB) plays an important role in stabilising the knee, especially during rotational movements. In a anterior cruciate ligament rupture the ALL is therefore often co-affected, which can contribute to increased knee instability.
In addition to a capsular structure, the indirect tendon itself has a fair amount of variation - both in properties and course. These variations are not considered separate tendons but may affect the injury susceptibility of the proximal rectus femoris.
Variations in the indirect tendon of the rectus femoris
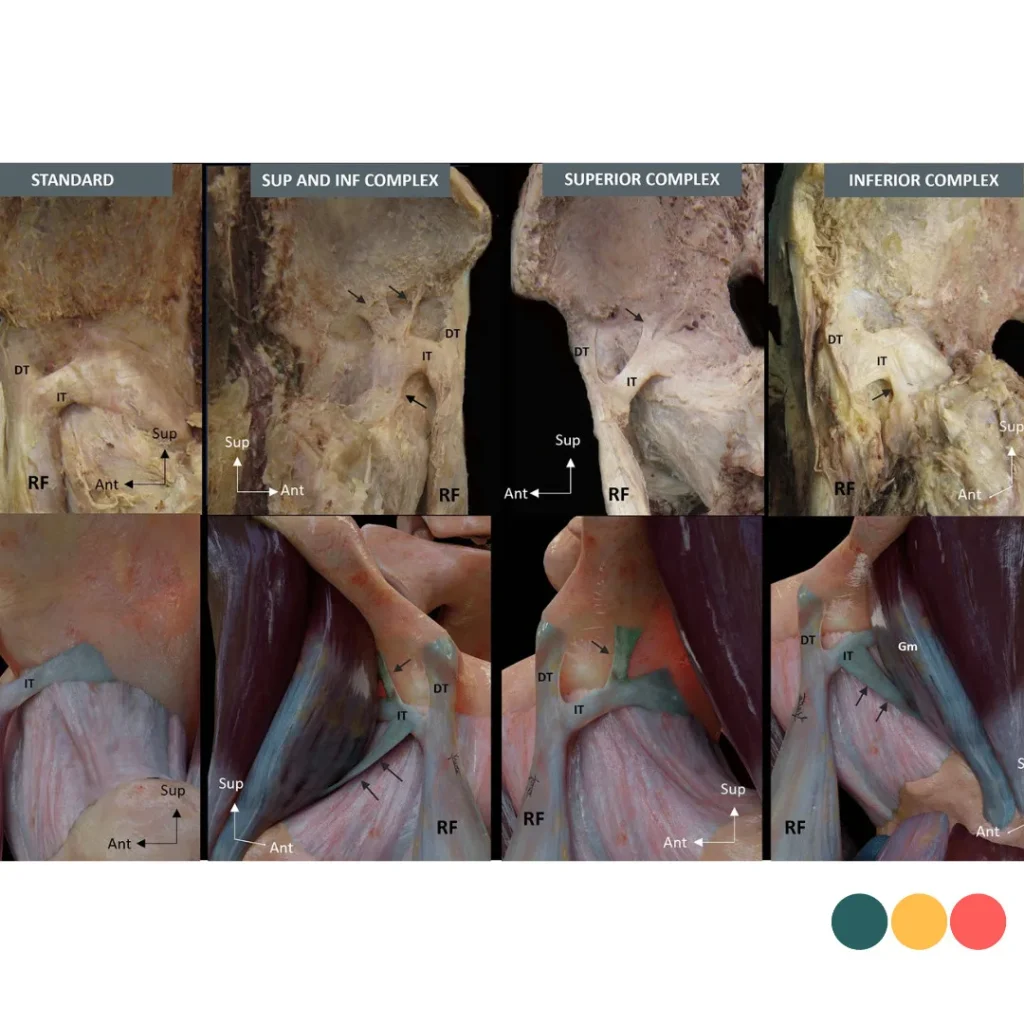
Anatomical examination shows that the attachment of the tendon of the rectus femoris often different from standard descriptions. In more than 60% of the cases, researchers found variations in the indirect tendon, which runs from the hip joint and is essential for force transmission.
In many of the cases, there were additional connective tissue connections from the tendon to surrounding structures. Based on this, we can distinguish between four main types, from a standard shape with no extra connections to tendons with extensions above, below or in both places.
The most common variations were an upper connective tissue connection to a groove at the hip joint (43.7%) and a lower extension - also known as the 'third tendon' - towards the gluteus minimus and the ligamentum iliofemoral (47.9%). In addition, in 39.6% of cases, the transition from tendon to muscle fibre started early, possibly affecting force distribution. While these variations have not yet been directly linked to specific injuries, they do suggest individual differences in tendon attachment and fascial connections. As in many other cases, more research is needed to better understand whether and how these anatomical differences contribute to injury risk and recovery.
Imaging in a rectus femoris injury
Although variations in the tendon structure of the rectus femoris do not usually cause symptoms, they can actually become visible and relevant when injured. A striking example is the bull's-eye phenomenon, a specific pattern found on both ultrasound as MRI can be seen in central muscle injury.
This phenomenon occurs when the deep tendon fibres of the indirect head are damaged. On imaging, you then see a round or oval zone of fluid and swelling in the centre of the muscle, while the more superficial muscle layers remain largely intact. The result is a kind of notch in cross-section, with a dark centre and a brighter edge - hence the name bull's-eye.
During a echo we see a central, less reflective zone surrounded by normal muscle tissue. Although more subtle than on MRI, this pattern is easy to recognise, especially when the clinical picture indicates an acute injury after sprinting or a vigorous pedal stroke. This helps distinguish injuries of the central tendon from superficial muscle injuries, which are often milder and recover faster.
Interestingly, some anatomical variations are barely visible on imaging under normal conditions. Only when injured, due to associated swelling or bruising, do these structures become more apparent. This explains why certain injury patterns become visible only during the recovery process or on later imaging.
The picture just got a little more complete
The anatomy of the rectus femoris is richer and more complex than the classical model led us to believe for many years. In addition to the direct and indirect head, a third tendon structure appears to be present in many cases: the capsular head. This additional attachment from the hip capsule subtly joins the central tendon and often remains underexposed in standard anatomy.
Especially in muscle injuries that do not behave entirely by the book, knowledge of these variations can make all the difference. We now know that there is a clear distinction between superficial injuries and deep, central injuries of the rectus femoris - with major implications for recovery time, rehabilitation approach and likelihood of return to sport. Anatomical variations such as the capsular head may offer additional explanations for atypical imaging or unexpected recovery trends.
The more we know about the structure of this muscle, the better we can understand, classify and target injuries. Not only does this contribute to a more accurate diagnosis, it also helps us better tailor rehabilitation to the type of injury. And that ultimately benefits the recovery and also the athlete.

Related complaints
Proximal hamstring complaints
Hamstring injuries are common in athletes. Quick action and targeted Physiotherapy can...
Achilles tendon rupture
A complete rupture of the Achilles tendon often occurs during explosive movements where there is a sudden application of a lot of force,...