From first signs to stress fracture
Bone stress injuries (BSI) is the collective term for all overuse injuries of the bone. This is a broad spectrum of reactions caused by an accumulation of minor damage in the bone tissue. From mild stress reactions with only some oedema in the bone, to complete stress fractures. These stress fractures account for about 20% of all BSI. Here, an actual fracture line is visible on the radiograph. These injuries occur broadly in two ways: by high loading on healthy bone (too much, to soon, to often), or by normal loading on weakened bone, as we often see in athletes where energy deficiency leads to reduced bone density. Runners are particularly affected by this injury. As many as 50 to 75 per cent of all bone stress injuries occur in running. The repetitive shock loading, combined with often high training volumes, makes running especially vulnerable. Interestingly, female athletes are two to four times more at risk than their male counterparts. This difference becomes even more pronounced when there is an energy deficit. A problem that is unfortunately still too common in sports where body weight still clearly plays a role.
A recognisable pressure pain over the affected bone is generally the main signal of a bone stress injury. A traditional radiograph is often the first imaging step when these symptoms are suspected. For a more focused diagnosis, especially in the stages before an actual fracture, MRI is the gold standard. It also gains ultrasound to popularity, especially as a first option given its accessibility and safety. Once a BSI is diagnosed, early action is important to reduce pain and promote healing. The severity and, in particular, the location of the injury determine further management. Low-risk locations are usually treated conservatively, while high-risk areas require direct referral to orthopaedist in some cases. Prevention of bone stress injuries mainly focuses on recognising and adjusting modifiable factors such as diet, lifestyle and exercise load.
The fine line between adaptation and repair of bone tissue
The strength of bone lies in its ability to adapt to mechanical loads. According to Wolff's law, a fundamental principle in biology, the structure and density of bone continuously adjusts based on the forces acting on it. This happens through a dynamic system in which osteoblasts (bone-building cells) and osteoclasts (bone-degrading cells) work together in a continuous interaction of breakdown and construction. With every workout, every jump, every landing, this system is activated.
This adaptation process is normal and even desirable. Minor damage that occurs during strenuous exercise is part of this natural cycle. With sufficient rest, the bone not only repairs itself but gets stronger. Strength training and also other forms of physical training increase bone density. Only a problem arises when the balance here gets upset. Then micro-damage accumulates faster than it can repair.
A spectrum from warning to breaking
There is not yet a good Dutch translation for the broader term bone stress injury. But the scientific literature does make a sharp distinction between initial signs of bone overload, which can lead to a stress fracture. A stress fracture is just the final stage within the whole continuum of overuse injuries to the bone. A bone stress injury is thus the umbrella term for any stage of overloading the bone. It starts with irritation of the bone tissue. On an MRI, you may then see increased activity of blood vessels and some fluid around the bone, but the structure itself is still completely intact.
If the stress lasts too long or recovery is insufficient, irritation builds up in the hard outer layer (cortex) of the bone. Only then do we speak of a true stress fracture with an actual fracture line on imaging. Recovery requires considerably more time, often months rather than weeks.
Relative energy deficiency in sport
Relative Energy Deficiency in Sport (RED-S) is a complex syndrome that occurs when athletes structurally consume more energy than they take in. It is not about not eating enough alone, but a deficiency of energy intake compared to training load. This deficit affects almost every system in the body: from hormone balance and immune function to bone metabolism and muscle recovery.
In the past, people mainly talked about the Female Athlete Triad, which was characterised by low energy intake, menstrual disorders and reduced bone density. But we know that these symptoms are not limited to women.Now we know that RED-S also affects male athletes, often without obvious hormonal warning signs. The body reacts to energy deficiency by conserving energy in non-essential processes. The result is reduced performance, slow recovery, irritability and an increased risk of injuries such as stress fractures. This risk is up to three times higher than in athletes with a healthy energy balance.
The paradox of RED-S is that it occurs precisely in disciplined, performance-oriented athletes. They train hard, eat seemingly healthy food, but do not replenish their energy reserves sufficiently. Especially in sports where weight or endurance are crucial such as running, cycling, gymnastics, this danger lurks. Recovery requires more than just extra calories. Recovery requires more than just screwing up calorie requirements. It requires awareness, adjustment of training load and guidance from professionals such as (sports) dieticians, physiotherapists and doctors. The aim is to rebalance energy intake with load, giving the body renewed space to perform, recover and adapt to the desired load.
Fredericson grading, not a black-and-white diagnosis
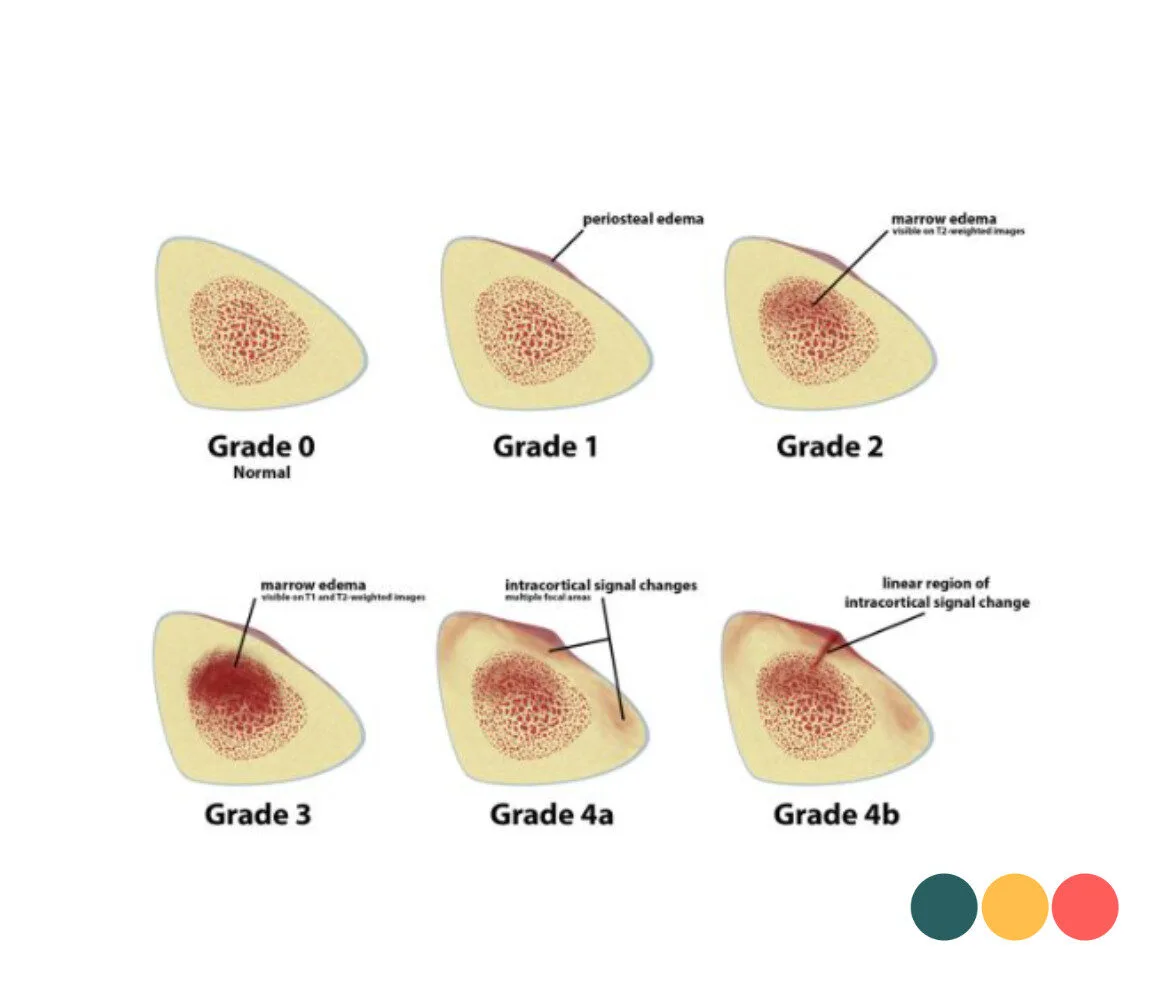
The Fredericson grading helps us better understand what stage an impact stress injury is at, from an initial warning to an actual fracture. The grading was created based on MRI images. An MRI has different settings to make certain structures more visible. T1 images mainly show the structure and build-up of the tissue. Think here of the shape of the bone, for example. T2 images along with the so-called STIR images are instead sensitive to fluid and inflammation. With structural overload, we often see a lighter, more clear signal, indicating fluid accumulation or tissue reaction. Together, these images give a good picture of how active the injury is and how far the process has progressed. With mild overuse, you see mostly changes inside the bone (the bone marrow), but as the injury gets worse, the bone membrane (periosteum) and eventually the hard bone wall (cortex) also get affected.
The four gradations according to Fredericson:
- Grade 1: A mild bone marrow reaction, visible as an increased signal on T2 or STIR (fluid accumulation) images, but no abnormality yet on T1. This is the earliest stage of overload.
- Grade 2: An abnormality is visible on both T2 and T1 images. This means that the bone marrow contains more fluid and the structure of the bone has already changed.
- Grade 3: Besides bone marrow oedema, the bone membrane (periosteum) is also inflamed or irritated. Sometimes you can already see incipient damage to the outer bone layer.
- Grade 4: A clear fracture line is visible in the cortex. This is the final stage of this continuum, or a true stress fracture.
The higher the grade the longer recovery will take. A grade 1 or 2 injury often recovers with temporary adjustment of training and rest, while grade 3 and 4 injuries require a longer period of relief. In practice, an MRI is not routinely performed on athletes with suspected similar symptoms. This is mainly due to cost, waiting times and limited availability. Moreover, an MRI only provides really valuable information if the injury is already more advanced. Ultrasound can often provide the right direction with a first look. Here, we look at the reaction of the periosteum, fluid accumulation or tendon irritation near the painful area. This gives a good, initial insight into the severity of the injury and helps to make targeted load adjustments, without requiring an MRI right away.
The difference in location of stress fracture
A recent meta-analysis of Hoenig et al. (2022) and Eissele et al. (2023) show that the location where the bone stress injury is located greatly affects the duration of recovery. These studies show a huge difference in recovery time between different locations. A stress injury in the tibia recovers in 44 days on average, while the exact same grade of injury in the navicular bone of the foot takes 127 days on average, almost three times as long. And these are still only averages; the actual spread lasts from a few weeks to more than half a year.
These major differences have everything to do with the unique characteristics of each bone. The tibia and fibula are well supplied with blood and have favourable biomechanical conditions. This blood supply provides oxygen and nutrients essential for recovery, while the relatively straight force transmission evenly distributes mechanical stress. Injuries here usually heal within six to eight weeks with relative rest and appropriate training.
But in the high-risk zones, it is a different story. The navicular bone in the midfoot, the base of the fifth metatarsal, the femoral neck, and the anterior side of the tibia - these locations combine limited blood flow with high mechanical stress. The navicular bone, for example, sandwiched between other foot bones, receives blood through only one smaller blood vessel that is easily compressed during loading. At the same time, this tiny bone has to absorb enormous forces with each landing. The result is slow, laborious healing with a constant risk of complications such as non-union (non-healing fracture) or avascular necrosis.
When groin pain goes wrong
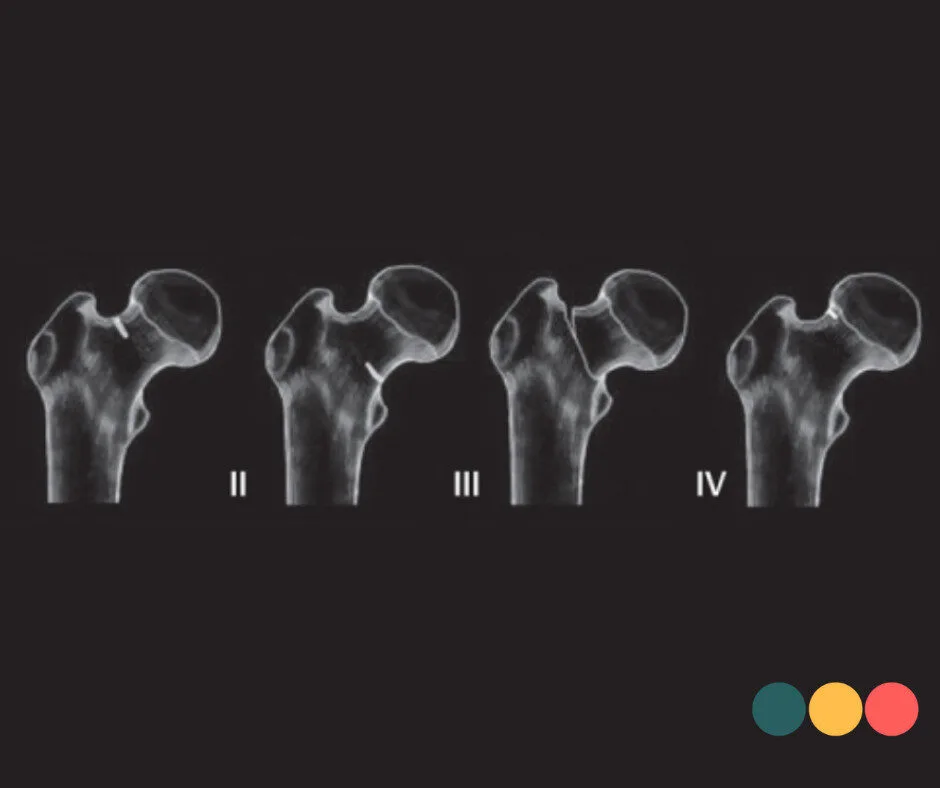
Of all the high-risk sites for a bone stress injury, the femoral neck, the narrow piece of bone between your hip head and thigh, is perhaps the most feared. Although this injury accounts for only 3% of all stress fractures in athletes, the consequences can be major. This injury was first described by German army doctors as early as 1905, but it is only since the 1990s that we have seen it increasingly in athletes as well, rather than just military personnel. The figures do not lie: half of all athletes who suffer this injury never return to their former level. In the case of a displaced fracture this even rises to 60%. In contrast, in early detection, when the fracture has not yet been displaced, almost 100% can recover completely without permanent damage. With a displaced fracture, avascular necrosis can occur in over 40% of cases. This is the death of the hip head due to lack of blood supply. For a young athlete, this can mean total hip replacement.
The femoral neck is especially vulnerable due to its anatomy and the large forces acting on it. With every step during jogging, this part of the hip has to absorb forces of three to five times your body weight. Most of these are compressive forces on the inside (bottom) of the neck. But on the outside (top), tensile forces are actually created by the bending of the bone. Imagine a stick that bends a little.
The difference is in the direction in which these cracks grow. A compression fracture on the inside grows obliquely (45 degrees) through the bone, producing a relatively stable fracture. The fracture parts are pressed together, so they usually do not shift as long as the fracture is less than half the width of the neck. With no loading and rest, it usually heals without surgery.
But an exterior tensor fracture develops at a 90-degree angle through the bone. This creates a transverse, unstable fracture line. When loaded, the fracture parts are pulled apart rather than compressed. The risk of displacement is much higher, and with it the risk of avascular necrosis. Every week of missed diagnosis dramatically reduces the chances of full recovery. Awareness among athletes and health professionals can make the difference between a temporary interruption or the permanent end of a sports career.
Physiotherapy for stress fracture
Recovering from a bone stress injury requires understanding the process of strain and recovery. The body signals in time when the recovery phase has been too short or the load too high. Not by stopping everything but by adjusting movement and training to what the body can handle at that moment. Bone recovers in stages and needs time to come back stronger. You cannot speed up bone recovery, you can only slow it down. When we respect that principle along with structured Physiotherapy it creates space again for recovery, confidence in the body and a safe return to sport.
