Pain on your tailbone, coccydynia
Tailbone pain, also known as coccydynia called pain, is an annoying complaint that can significantly hamper daily functioning. The pain is at the bottom of the spine, at the tailbone (coccyx) and was first described in 1859. It usually involves a sharp or nagging pain that increases when sitting, standing up or cycling and sometimes radiates to the lower back or pelvis. The causes are diverse: a fall on the tailbone, long-term stress on the tailbone, being overweight or the natural shape of the tailbone can contribute to the onset of symptoms. Pregnancy and especially childbirth are also common reasons for complaints in this region. During pregnancy, hormonal changes cause increased mobility of the pelvis. The tailbone can come under considerable pressure during childbirth, causing irritation or even a change in position. Treatment of coccydynia depends on the cause and severity of the symptoms. Sometimes giving advice and adjustments in daily life is enough, but manual therapy, exercise therapy are also treatment options within Physiotherapy. Should this not have the desired result, local injections or, in rare cases, surgery may be part of a treatment plan. At Physio Vital together, we look at an appropriate approach aimed at relieving pain and restoring normal movement.
What does coccydynia really mean
The word 'coccydynia', first used by Simpson in 1859 and derived from the Greek 'coccyx' (referring to its resemblance to a beak) and the suffix '-dynia', meaning pain in the Latin language. Despite the condition being recognised as early as the 18th century, many questions remain to this day about the cause of the pain, risk factors and the results of various treatment methods.
In this text, the terms coccyx, coccyx and tailbone used interchangeably. They all refer to the same part of the body: the lower, often small and triangular part of the spine located just above the buttock cleft. Medically, the term coccyx used, while in everyday language coccyx or tailbone are more common.
Anatomy of the tailbone
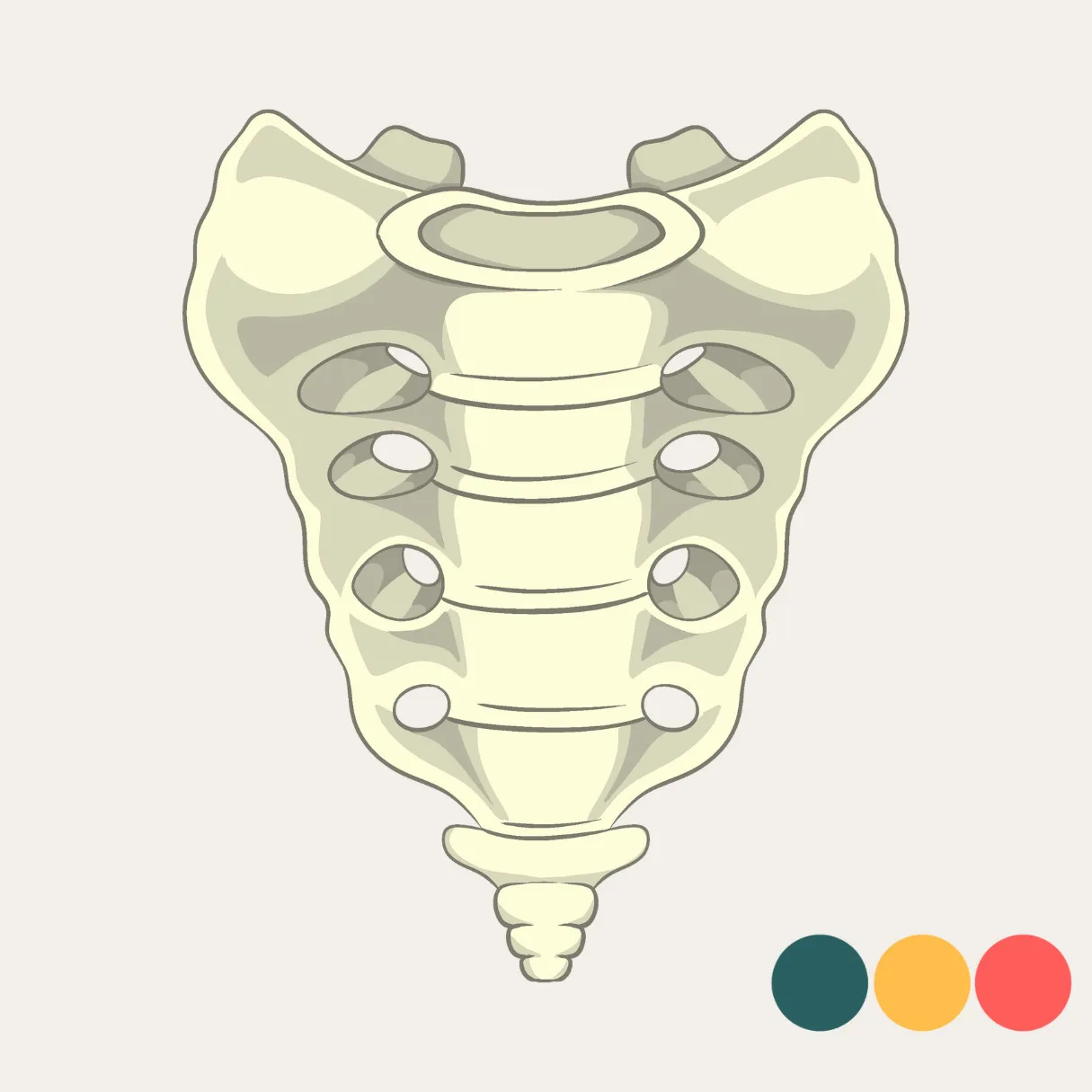
The coccyx - or coccyx in medical terms - forms the lower end of our spine. It consists of three to five smaller vertebrae, which in most people are partially or fully fused together. The upper part of the tailbone makes the upper joint with the sacrum. Small intervertebral discs may still be present between the vertebrae of the coccyx in some cases. These intervertebral discs vary greatly in shape, sometimes they are still intact, sometimes they have changed into cartilage-like structure or fatty connective tissue. This can cause the tailbone to move too much in some cases but also to move too little.
At the front of the tailbone are the attachments of important structures such as the pelvic floor muscles (including the levator ani) and ligaments. The back can be recognised by the small protrusions that, together with the sacrum, form a kind of opening through which a nerve branch, the fifth sacral nerve, runs. The sides of the tailbone provide attachment sites for various muscles and ligaments, such as the gluteal muscles and the other ligaments that stabilise the pelvis. Also located here is the muscle called the iliococcygeus, which is important for supporting the pelvic floor and controlling bowel movements. Although a small part of our body or spine itself, abnormalities in its shape or mobility can lead to pain and restrictions, especially during activities such as sitting or standing up.
A fall as the main cause
The most common cause of coccydynia is a moment of trauma, often in the form of a fall directly on the buttocks. While sitting, the tailbone, together with the ischial tuberosities, forms one of the three supports of the body. This position makes it particularly vulnerable to direct pressure or impact. It is estimated that between 50 and 65 per cent of people with tailbone pain have a history with a fall or similar moment. The severity of the injury can then range from mild muscle damage or irritation to fractures or subluxations (dislocations) of the coccyx.
Prolonged sitting on hard surfaces can also cause symptoms. In older literature, this was sometimes referred to as the 'television disease', referring to people sitting still for hours in a particular sitting position. Internal trauma such as that caused by complicated or instrumental deliveries can also be a source of tailbone pain in women.
If the pain persists for a long time despite treatment and appropriate advice, it may be wise to conduct further investigations. In most cases, this is not necessary, but it does help to rule out other, less common causes and thus arrive at an appropriate approach. Recovery is often slow, even with appropriate advice and management. It is not unusual for it to take several months before there is clear improvement. And in some cases, recovery can even take up to a year. Patience, a step-by-step approach and taking the symptoms seriously are essential here.
Influence of physique and gender
Being overweight is a known risk factor in tailbone pain. With obesity, there is often a different sitting posture and limited pelvic mobility, putting extra pressure on the tip of the tailbone. This leads to increased mechanical strain while sitting. A BMI above 27.4 in women and 29.4 in men is considered in the literature to be a factor for developing coccydynia.
In addition, studies show that women are affected about five times more often than men. This is due to several factors, women naturally have more ligamentous laxity, a different pelvic position and undergo more frequent stress on the pelvic region during pregnancy and childbirth.
Abnormal shape of the tailbone
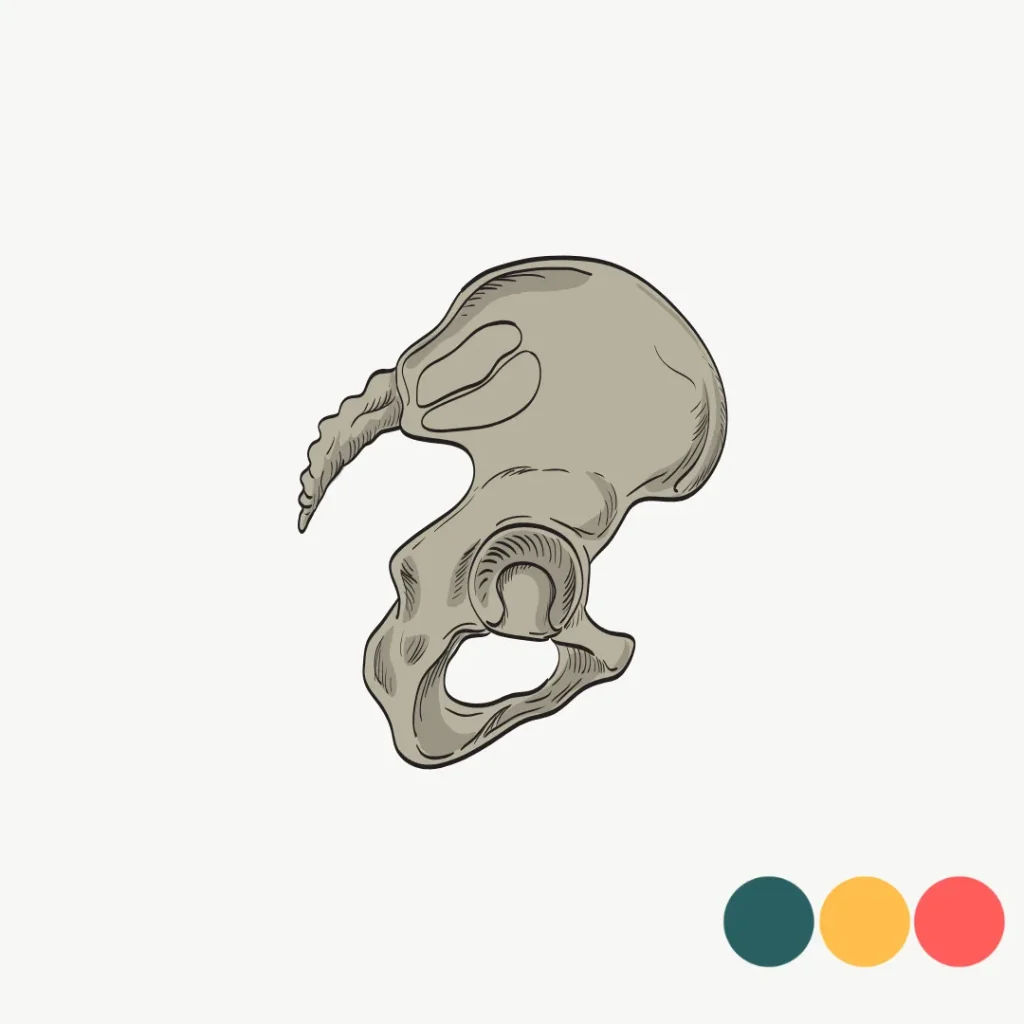
The shape of the coccyx varies greatly from person to person. Six different morphological variants have been described in the literature. Some coccyxes are straight or slightly curved forward, while others curve sharply forward or even backwards. A lateral position can also occur. And as with other structures in our bodies, this can be quite normal. We are not a car that is supposed to be neatly aligned. But when the anatomy is way out of average, it can be a reason for complaints. Especially the types with an acute angle, subluxations or a point pointing backwards are often seen in people with coccydynia.
The spiculum
A bony protrusion at the end of the tailbone - also called a spiculum called - is not always present, but is seen more often in people with coccydynia than in those without symptoms. The literature shows that about 14% of patients with tailbone pain has a spiculum. This small bone point can in some cases cause irritation of surrounding tissue, such as tendons, muscles and bursae (bursae), leading to a persistent bursitis (adventitial bursitis).
However, it is important to stress that not everyone with coccydynia has a spiculum, and also that not every spiculum automatically causes symptoms. The degree of irritation depends, among other things, on the position of the tailbone, its mobility, the pressure applied to it when sitting and the sensitivity of the surrounding tissues.
Abnormal mobility of the coccyx
Coccydynia is increasingly considered a dynamic problem. In many people with coccyx complaints, the mobility of the coccyx is greater than normal. During sitting, the coccyx is supposed to flex slightly. However, in about 69% of cases, there is greater than average range of motion. Or an excessive flexion of more than 25 degrees. On the other hand, the tailbone can also be too rigid. Here, the tailbone moves less than 5 degrees and is actually very stiff. Normal mobility is described as movement between 5-25 degrees
A distinction can thus be made between different forms of mobility: a luxation (posterior subluxation), hypermobility (excessive motion), immobility (stiffening), or normal mobility. Such abnormalities can be well visualised through dynamic imaging, such as X-rays in sitting and standing positions.
Wear and tear of intervertebral discs
Between the small vertebrae there are remnants of intervertebral discs in some people. These structures are not present in everyone and vary greatly in shape and composition. Sometimes they are still reasonably intact and in other cases they have been partially replaced by cartilage, connective tissue or fatty tissue. Under the influence of normal ageing, repeated mechanical strain or an experienced trauma, these intervertebral discs can show wear and tear. When these structures cause pain, we speak of discogenic pain.
Discogenic pain at the tailbone is thus caused by wear and tear of these intersegmental structures. It is a possible explanation for symptoms when other causes such as trauma or abnormal mobility are not immediately apparent. Examination with contrast medium (discography) or examination after surgery shows that intervertebral disc wear is present in about 40% of people with coccyx pain.
Although this type of pain is difficult to demonstrate precisely, wear and tear of the intervertebral discs remains a major concern in cases of persistent or persistent tailbone pain. A careful interview, physical examination and any additional tests are then essential for proper treatment.
What do you feel with coccydynia
Although coccydynia is usually caused by mechanical or anatomical factors, such as a fall or abnormal position of the coccyx, other causes also occur in rare cases. These include inflammation, benign tumours or calcium deposits around the joints of the coccyx. These are rare, but can sometimes be the reason for persistent pain symptoms.
Further investigation for tailbone pain
In case of persistent complaints, imaging valuable to better identify the cause. X-rays (standing and sitting) or a CT scan can show abnormalities in the position or shape of the coccyx, such as subluxations or curvatures. An MRI is especially appropriate when muscle or tendon irritation, inflammation or wear and tear of the bone is suspected.
When in doubt about the mobility of the coccyx, dynamic radiography can be used. This involves taking X-ray images in different positions to assess the movement of the coccyx during sitting and standing. Although this technique can provide valuable information, its interpretation is difficult due to the lack of a standardised method.
Ultrasound offers many advantages in daily practice. It is an approachable, quick and safe way to assess the structures around the tailbone. Bursas or muscle and tendon swelling can be well mapped. In addition, ultrasound can provide early information on the shape, position and possible irritation of the coccyx. This makes it a valuable tool in the initial assessment of symptoms.
Physiotherapy and other treatment for coccydynia
Treatment of coccydynia usually proceeds in stages, starting with simple, non-intrusive measures. Adjusting sitting posture and using a special pillow can provide relief. It is also useful to limit prolonged sitting wherever possible. Painkillers or anti-inflammatories can be used temporarily to make the symptoms more bearable.
Physiotherapy and manual therapy can help improve the mobility of the tailbone and reduce tension in the surrounding region. By treating the area around the lower back and pelvis, the stress on the tailbone can be reduced. The aim of physiotherapy is to restore movements of the pelvis and spine to as normal and pain-free a state as possible.
When this treatment strategy is insufficiently effective, an injection may be considered. Here, anti-inflammatory medication is administered to the painful area or all around in the pelvic region. If the pain persistently recurs, other techniques such as prolotherapy or nerve treatment may also be considered. The effectiveness of prolotherapy in coccydynia is still limitedly substantiated. Although some small studies show positive results, such as pain reduction after injections with a glucose solution, large-scale well-designed scientific studies are lacking. The studies that do exist often have a small sample size, lack control groups or use different protocols, limiting reliability.
Surgery, such as the removal of (part of) the tailbone, is only considered if all other treatment options have given insufficient results. Although the results may be good in select cases, it is important to remain critical. Not all pain at the tailbone is actually caused by the bone itself. Sometimes the cause lies in surrounding tissue or in the way the body moves and loads. In such cases, surgery may not have the desired effect. In addition, it is a surgery with an increased risk of wound problems because of its location. A careful course of action beforehand is therefore very important to determine whether surgery is really appropriate.
Don't let your complaints sit idle! There is almost always a suitable solution
Coccydynia can be long-lasting and frustrating, but the good news is that in most cases something can be done about it. Although recovery can take considerable time, sometimes several months to even a year, there are clear steps that can bring relief. From simple adjustments in sitting behaviour to targeted physiotherapy. Treatment options are versatile and often effective. The important thing is not to just sit out the process, but to actively seek appropriate help. With the right guidance, careful analysis of the cause and a tailor-made plan, improvement is almost always possible. So don't linger too long with symptoms, but consult a professional familiar with this condition.

Related complaints
Proximal hamstring complaints
Hamstring injuries are common in athletes. Quick action and targeted Physiotherapy can...