From Munich to Barcelona, another look at muscle injuries
Muscle injuries are the most common sports injuries. They often occur during explosive movements such as sprinting, jumping or sudden braking. The muscles of the upper leg are particularly vulnerable, especially the hamstrings at the back and the quadriceps At the front - including the rectus femoris.
Muscle injuries can range from mild muscle strains to complete ruptures. Although muscle tissue generally has good restorative capacity, in some cases the recovery process rarely proves straightforward. At first glance, recognising, interpreting and managing muscle injuries seems like a routine process. Yet beneath the surface, a deeper complexity lurks. These differences are anything but purely academic and have a major impact on safe and effective rehabilitation and reducing the risk of future injury.

Location makes a difference
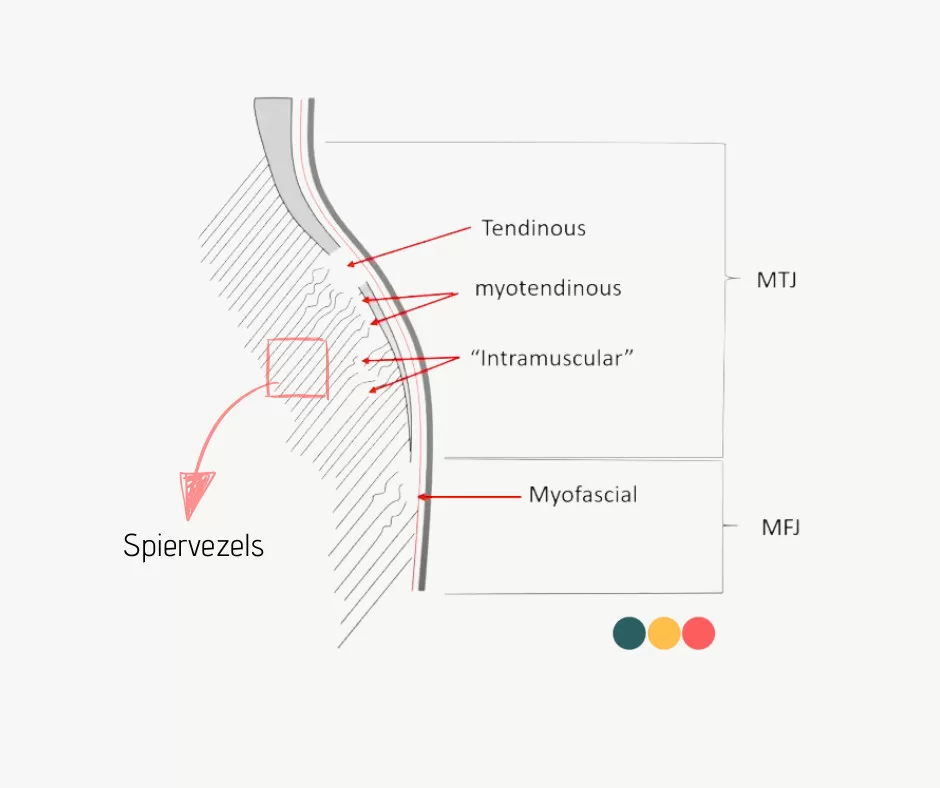
A muscle is not simply a block of muscle fibres. Within the muscle tissue is a network of connective tissue structures - such as the endomysium, perimysium, epimysium and the central tendon (aponeurosis) - that together ensure the transmission of force. This connective tissue surrounding the actual muscle fibres functions as an internal skeleton of the muscle and forms a gradual transition between muscle and tendon.
Due to new insights into connective tissue architechture, we distinguish between different parts in the muscle, namely: tendinous, myotendinous, intramuscular and myofascial. This classification is not only clinically relevant, but is also increasingly supported by new insights into muscle anatomy and connective tissue architecture. Many muscle injuries occur at the transition between the muscle and the tendon, where the force from the muscle is transmitted to the tendon tissue.
Tendinous injury
This type involves damage to the central tendon or aponeurosis within the muscle. Tendon structures are poorly perfused, contain little elastin and regenerate more slowly than muscle tissue. Injuries at this level tend to heal slowly, have an increased risk of fibrosis formation and have a higher risk of recurrence.
Myotendinous injury
Here, muscle fibres become partially detached from their anchorage to the tendon or aponeurosis. This type of injury usually occurs during explosive or eccentric loading, such as sprinting or abrupt braking. The transition from muscle to tendon is more complicated than we thought. There are multiple zones in it where force is transferred Precisely those spots turn out to be especially vulnerable during sudden, large loads such as sprinting or braking.
Intramuscular injury
This type involves damage within the muscle belly, away from the tendon structures. Recovery is usually more favourable because of blood flow and the good repair ability of muscle tissue. Nevertheless, it appears that larger intramuscular injuries can scar if there is insufficient build-up of load. In particular, large, centrally located haematomas can disrupt muscle architecture for a long time.
Myofascial injury
Here, the outer layer of the muscle is affected. These lesions often occur at the edge of the muscle, are usually superficial and highly visible in the form of bluish discolouration. Funnily enough, the prognosis is often more favourable, partly due to the good recovery ability of this area and low mechanical strain.
In particular, the tendinous and myotendinous injuries disrupt the force conduction of the muscle. Moreover, tendon structures have a poorer recovery capacity. This makes these lesions more susceptible to scarring, leading to reduced elastic capacity and increasing the likelihood of recurrence. The more these connective tissue structures are affected, the higher the likelihood of long-term loss of function and delayed recovery. The swelling or discolouration may be minimal, while the injury is more serious and has a major impact on the prognosis. It is precisely in this transitional area that many of the most clinically relevant muscle injuries occur. They are often more difficult to treat, have an increased risk of scarring and require careful, phased rehabilitation. The focus within this rehabilitation is on stimulating connective tissue repair, preventing overuse and building functional load capacity step by step - with particular attention to timing, monitoring and control of exercise load.
From Munich to Barcelona, limitations of existing classification systems
Traditionally, muscle injury is classified according to a three-step model: grade I (mild, no fibre rupture), grade II (partial rupture) and grade III (complete rupture). It is mainly based on the degree of visible damage, but takes little account of the precise location of the injury or the type of tissue involved as described above. As a result, important nuances - especially in the transition area between muscle and tendon - often remain underexposed, while this is precisely where many clinically relevant injuries occur.
In recent years, therefore, significant strides have been made in the development of more sophisticated classification systems that do more justice to the functional and anatomical complexity of muscle injuries.
Munich Consensus Statement (Müller-Wohlfahrt, 2013)
This classification represented a major advance in clinical thinking about muscle injuries. For the first time, a distinction was made between functional muscle injuries (without structural damage) and structural muscle injuries, with further subdivision into subtypes. This provided a useful basis for clinical reasoning, but still lacked depth at the anatomical level. For example, the exact location within the muscle-tendon continuum was not yet taken into account.
British Athletics Classification (Pollock et al., 2014)
The British Athletics Association introduced a more anatomically based classification and for the first time named the term intratendinous muscle injuries - injuries to tendon structures located ín the muscle tissue. An important insight, because anatomical research shows that tendons or aponeuroses do not end abruptly where muscle tissue begins, but gradually overflow into the contractile part of the muscle. As a result, many injuries occur at the interface of muscle and tendon tissue - so-called myoconnective injuries. This type of injury has important clinical implications, as recovery is slower and the risk of relapse is higher than for purely muscular injury.
FC Barcelona Classification (Valle et al., 2017)
FC Barcelona's system builds on previous models and adds additional dimensions such as injury mechanism (e.g. sprint-related), anatomical location, severity (in degree of fibre disruption), and risk of recurrence. Since 2019, within this classification, the intratendinous subtype explicitly named. Although this classification is very detailed and does much justice to the clinical complexity of muscle injuries, it is often difficult to apply in practice without access to advanced imaging and in-depth anatomical knowledge.
These modern classification systems have significantly deepened our understanding of muscle injuries. From a simple scale based on injury size, it has evolved to anatomically and biomechanically based models that do more justice to the complexity of muscle injury. However, the search for the balance between theoretical comprehensiveness and practical applicability remains. The challenge lies in being aware of these insights without losing the overview.
A look inside the muscle, how imaging helps diagnosis
In daily practice, ultrasound a widely used tool in the assessment of muscle injuries. It is approachable, quick to use and particularly valuable for mapping acute injuries. Ultrasound works on a grey scale basis and notably shows fluid, oedema and bleeding - signals indicating a tissue response after damage. In doing so, it offers a indirect but clinically useful image of the situation. Although we cannot see exactly which structures have been damaged, we do get information about the severity and course of the injury.
MRI is generally considered the gold standard, especially in the first 72 hours after muscle trauma. It provides accurate information about the type of tissue, the exact location of the injury and the involvement of the connective tissue skeleton surrounding the muscle fibres. But in practice, it is not realistic or necessary to put every athlete or patient directly under the MRI. MRI is costly, of limited availability and usually reserved for elite sports environments or complex cases.
This is precisely why ultrasound a valuable and viable alternative, especially in front-line settings. It allows therapists and doctors to quickly and effectively make an initial assessment and monitor the course of recovery. Yet ultrasound also has limitations: distinguishing between new injury and recurrence, for instance, is difficult, as both often show a similar picture of fluid and swelling - especially in the subacute stage, when clinical symptoms diminish but the tissue is still insufficiently load-bearing.
Most importantly, imaging never stands alone, but is always part of the complete clinical picture. Echo or MRI should therefore not be seen as the final diagnosis, but as a tool that, together with the patient's story (history), physical examination, strength measurements and functional tests, helps to reach an informed conclusion. Ultrasound in particular, if used properly, is a practical and reliable tool for assessing and monitoring muscle injuries - even outside top-level sport.
You win more with patience than with haste
Muscle injuries are among the most common injuries in sport. Although recognising such an injury often seems straightforward, the challenge lies in correctly interpreting the nature, location and severity of the injury and carefully planning the recovery process. New insights into anatomy, tissue repair and injury classification make it clear that muscle injury is much more than just the size of the injury.
With a good understanding of the biological phases of recovery, a clinically sound assessment of the injury type, and the thoughtful use of imaging and testing, we can significantly increase the chances of full recovery and sustainable sports recovery. And our message is: You win more with patience than with haste!

Related complaints
Achilles tendon rupture
A complete rupture of the Achilles tendon often occurs during explosive movements where there is a sudden application of a lot of force,...
Hamstring complaints in runners
Hamstring complaints are common among runners. Pain and loss of strength are common symptoms in hamstring injuries.