AC luxation: What is it and how to recover from it
An AC luxation, or acromio-clavicular luxation, is a common shoulder injury caused by a fall on the shoulder or a fall with a stretched arm. This injury occurs when the joint between the clavicle and the shoulder joint becomes damaged, often in combination with the tearing of ligaments. This can lead to a visible kicking position of the clavicle and symptoms such as pain, swelling and restriction of movement. This pedal position is also known as the piano-key phenomenon.

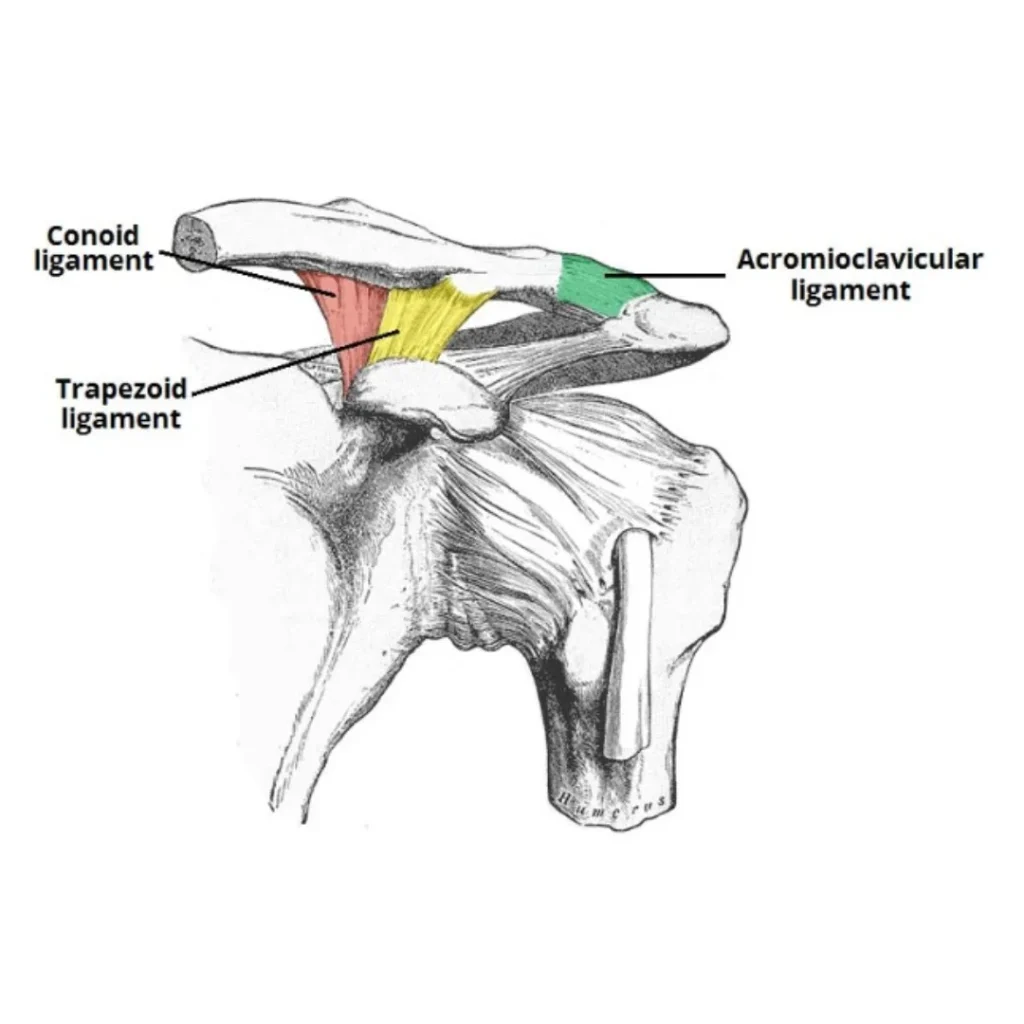
The anatomy of the AC joint
The AC joint forms the connection between the clavicle(clavicle) and the shoulder blade(acromion), stability is largely provided by ligaments. The acromio-clavicular ligament provides the direct connection between the two bone structures, while the other ligaments (trapezoid and coronoid ligament) give the clavicle even more stability to the shoulder blade. When these ligaments are damaged, the clavicle loses its support and can therefore move upwards.
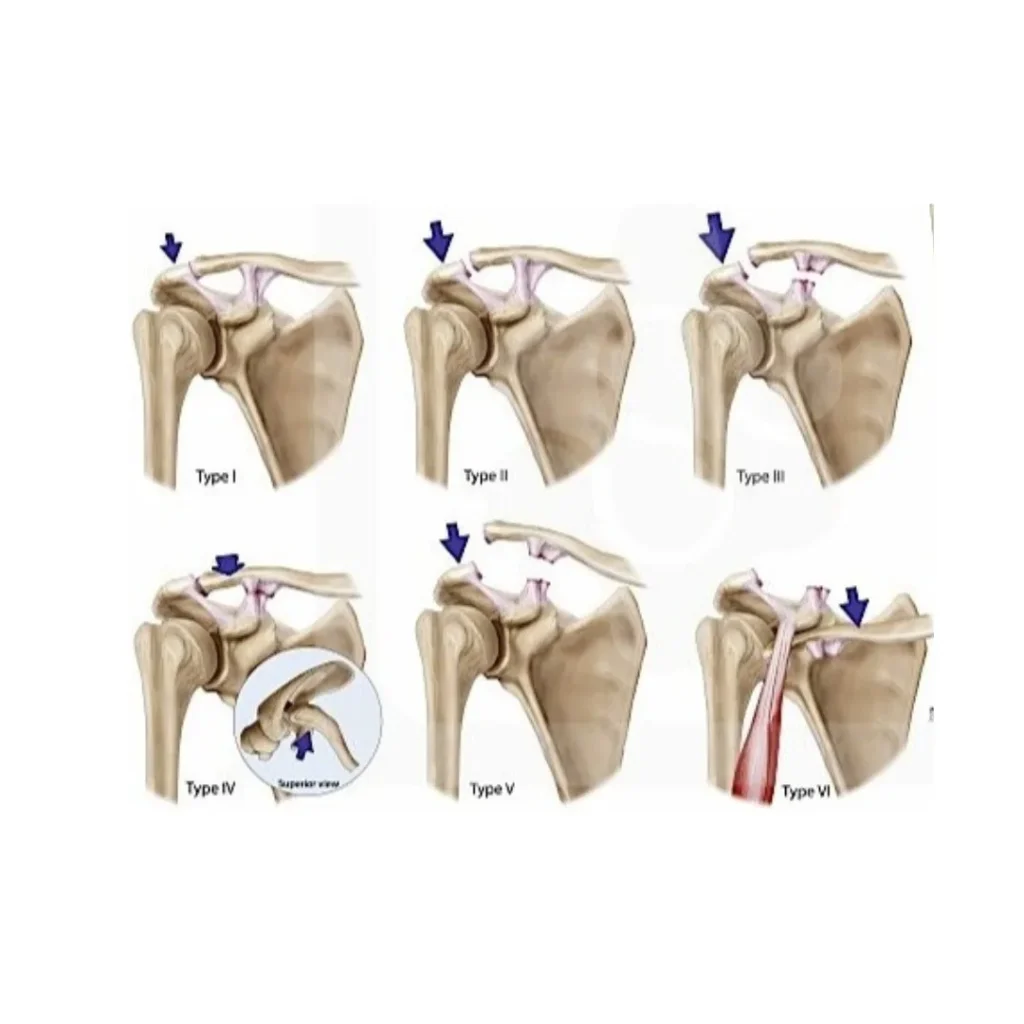
An AC luxation usually results from direct trauma, such as a fall on the shoulder during a sporting activity or an accident. The degree of damage to the joint and surrounding structures determines the severity of the luxation, which can range from a mild strain to a complete dislocation with muscle and tendon tears. See image for the different types of an AC luxation.
Symptoms and examination
A patient with AC luxation usually experiences immediate pain at the top of the shoulder, with the intensity depending on the severity of the injury. In addition to pain, there may be swelling and blue discolouration of the skin around the joint. In severe cases, a distinct deformity is visible, with the tip of the clavicle raised and forming a kicking position.
On examination, the 'piano key sign' is sometimes observed. This may involve pushing down the protruding end of the clavicle with pressure, after which it immediately springs back up. To determine the severity of the injury, imaging is usually used. X-rays or ultrasound examination identify the degree of dislocation and possible additional bone fractures.
Ultrasound can be a valuable addition to the diagnosis of AC luxation. This imaging examination allows not only to assess the position of the clavicle and the degree of luxation, but also to map any concomitant damage to ligaments, tendons and muscles. Unlike a standard X-ray, ultrasound provides a dynamic image of the joint in different positions, which helps map the function of the shoulder girdle. In addition, ultrasound is a quick, safe and non-invasive method that can be used directly in physiotherapy practice to better tailor the treatment plan to the specific injury and optimise the recovery process.

Treatment options depending on severity
The treatment of an AC luxation depends on the degree of damage to the joint and surrounding structures. For types 1 and 2, a non-operative approach is usually adopted. This involves immobilising the shoulder with a sling or sling for three weeks to give the damaged structures a chance to recover. In addition, painkillers and anti-inflammatories can be used to relieve symptoms. Once the first phase is over, physiotherapy can be started to increase shoulder mobility and build muscle strength. During the first six weeks, heavy loading of the shoulder girdle is not recommended to avoid complicating the recovery process.
In severe injuries, as in some grade 3 and almost all grade 4, 5 and 6 luxations, surgical intervention is often necessary. Surgery focuses on returning the clavicle to its correct position and stabilising the joint using fixation materials such as pins, screws or special stabilising cords. A well-known technique is the tight rope procedure, in which a strong wire is stretched between the clavicle and the coracoid protrusion to keep the clavicle at the correct height. This way, the damaged ligaments are given a chance to repair. If there is additional damage to the articular cartilage, an AC resection may be performed, in which a small part of the clavicle is removed to reduce pain.
Rehabilitation and functional recovery
The recovery process after AC luxation requires a structured approach to restore the functionality of the shoulder as soon as possible. Immediately after surgery or start of conservative treatment, pendulum exercises are started in hospital to prevent stiffness. In some cases, a frozen shoulder can develop if there is no regular movement in the shoulder joint. During the first three weeks, wearing a sling remains necessary to allow the ligaments to heal optimally.
After this initial phase, physiotherapy is carefully started, focusing on improving mobility and building muscle strength in a dosed manner. During the first six weeks, heavy loading and movements above shoulder height are avoided to prevent overloading the recovering structures. Exact treatment is tailored to the patient's individual situation, balancing sufficient rest and recovery with gradual loading.
Sports resumption strongly depends on the type of sport and the degree of recovery. Walking and cycling can often be resumed after only three weeks, provided the pain and swelling have subsided sufficiently. More strenuous sports, such as contact sports or strength training, require more recovery time and are resumed in phases in consultation with the treating doctor. In many cases, full functional recovery is achievable within three to six months, depending on the severity of the injury and the treatment chosen.
Practical advice for a smooth recovery
Driving a car is only justified again when the shoulder has sufficient mobility and strength to safely handle the steering wheel. In practice, this is usually around four to six weeks after surgery. The fixation material used, such as the tightrope, can remain in place permanently and does not need to be removed unless it causes permanent symptoms.
An AC luxation can be a nasty and painful injury, but with the right treatment and guidance, a good functional recovery is possible. It is important to start early to minimise residual symptoms. Do you have questions about your recovery process or want professional guidance? Contact Fysio Fitaal Tilburg for a personalised treatment plan and expert tailor-made guidance. Or read more about the most common shoulder complaints.

Related complaints
Shoulder pain
Shoulder problems are common. Sometimes shoulder problems are also a recurrent injury.
Shoulder luxation (dislocation)
A shoulder luxation is usually caused by a hard fall and is often accompanied by pain ...
Subacrominial pain syndrome (SAPS)
Complaints occur when lifting or turning the arm inward/outward and the...