Peroneal tendon injury: causes, diagnosis and treatment
Complaints of the peroneal nerve are a common injury on the outside of the ankle. We can also speak of a peroneal complex consisting of 3 different muscles: the peroneus longus, brevis and tertius. The function of these muscles is mainly to stabilise the ankle joint. Injuries to these muscles cause symptoms on the outside of the ankle or foot. Its complex location makes it difficult to properly assess this muscle. Ultrasound can shed more light on this in some cases depending on the location of the injury. We can roughly divide the peroneus longus muscle into 3 anatomical sections. The region of the lower leg, the ankle joint and the foot. Most injuries to the peroneus occur in the region of the ankle. As a result, injuries in the other parts are often not seen as an injury to the peroneal nerve. There can also be different anatomical variations, which can make a precise diagnosis difficult.
Anatomy and function of the peroneal muscles
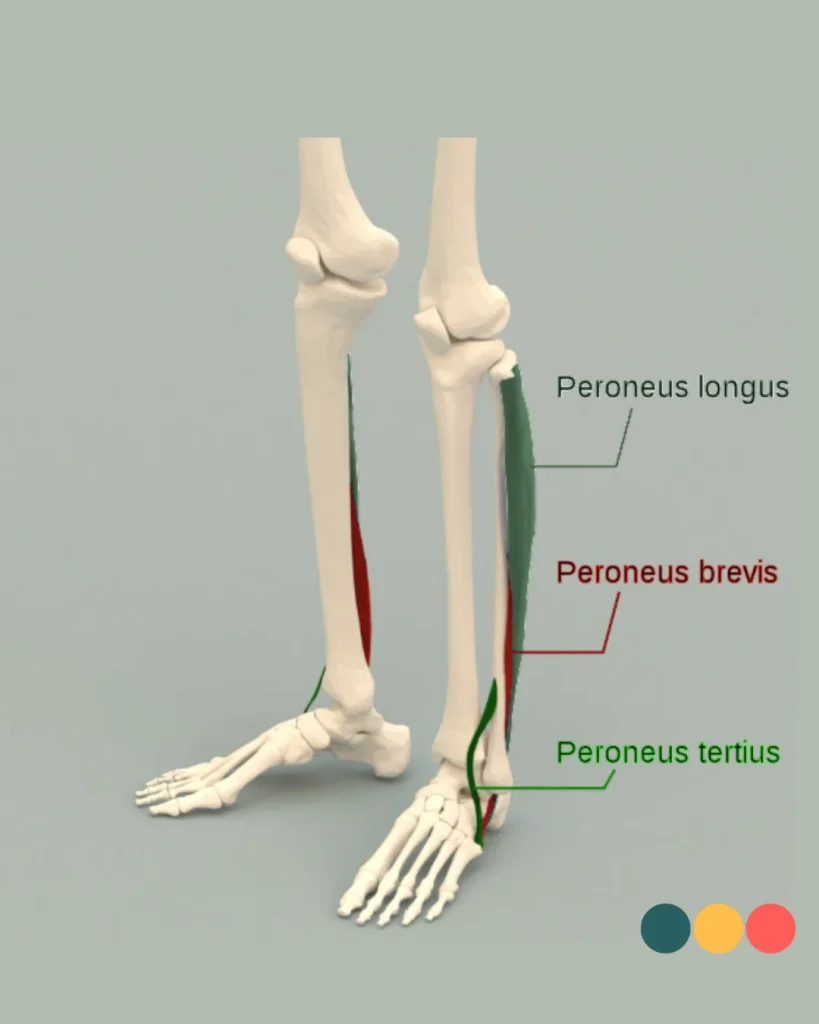
The Peroneus longus
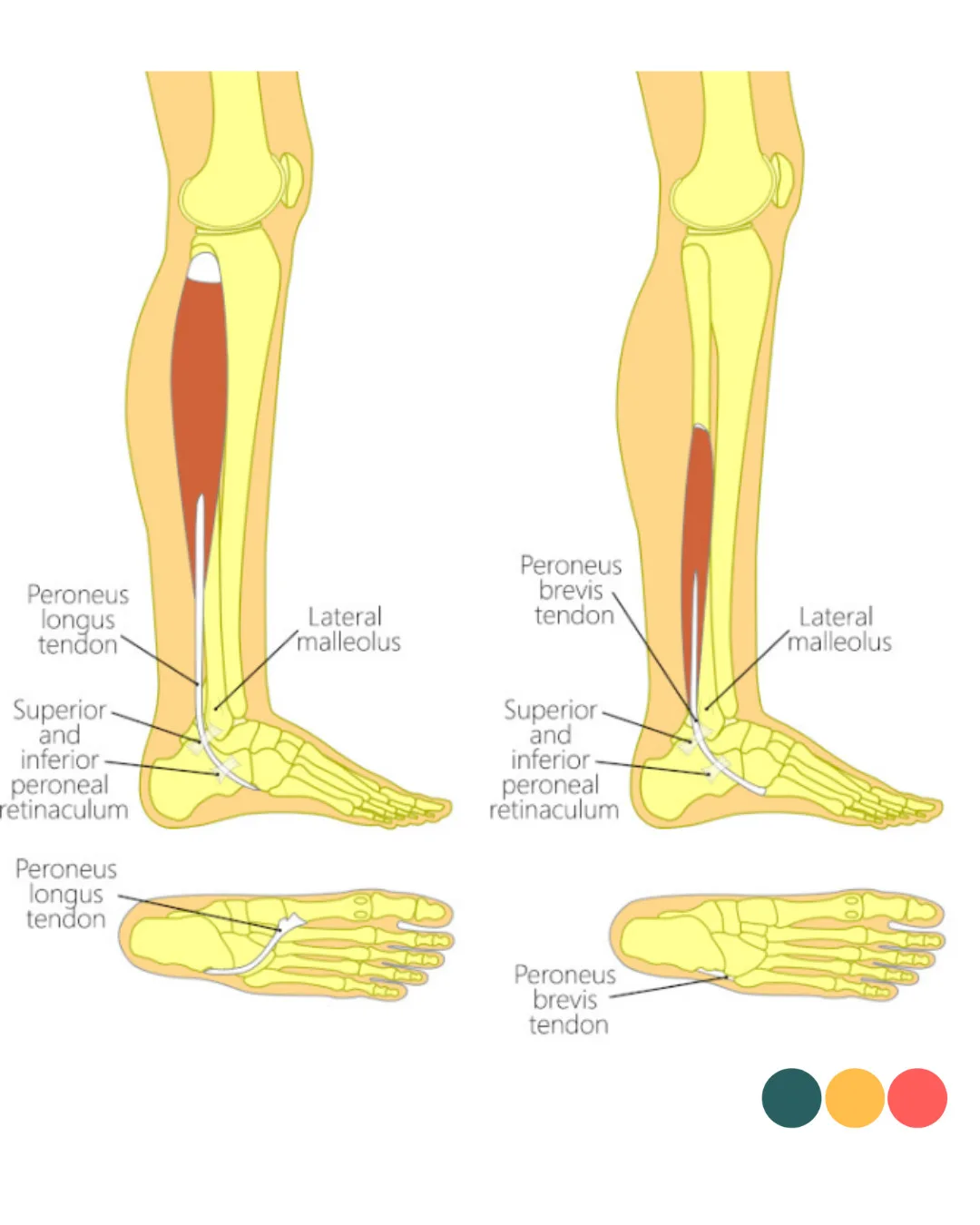
The plural of peroneus is peronei. The function of the peronei is eversion. In particular, it inhibits inversion (foot inwards) and this is precisely the movement you make when you sink through your ankle. Also, the peroneus makes plantarflexion (coming onto the toes) together with other larger muscles in the calf (soleus and gastronemicus). The muscle is located on the outside of the lower leg, also called the lateral side. The peroneus longus(long) has a long muscle tendon transition and starts well above the ankle. The course of the tendon section is long and complex. The tendon makes two sharp turns around the lateral malleolus and cubital tunnel and then departs to the underside of the foot towards metatarsal 1. The risk of injury to the peroneal tendon is also highest at these two locations because of high tensile forces on the tendon, especially in the cubital tunnel.As the peroneal longus runs under the foot, it is also very important in stability in the line of the big toe and metatarsal during walking.
The Peroneus Brevis
The peroneus brevis also originates well above the ankle joint on the fibula(calf bone). However, it is still below the peroneus longus that goes all the way to the fibula head to the knee. The peroneus brevis has a more direct course to the outside of the fifth metatarsal, the outside of the foot. An injury to the peroneus brevis is more common than to the longus. This is probably because the brevis lies between peroneus longus and the retro malleolar groove(protrusion on the outside of the ankle). During vigorous exertion, the tendon is pressed against the bone part and the risk of damage is simply higher. Like the other peronei, the peroneus brevis makes an eversion movement and is even the largest powerhouse of the 3. On average, we see that the peroneus brevis is responsible for more than 60% of force delivered. It also helps the large calf muscles with plantarflexion(coming onto the toes). With damage to the peroneus brevis, we see that the course of the peroneus longus becomes slightly forward towards the fibula(calf bone). Because of this mechanism, we see that the peroneus longus can also be damaged in the same way as described above with regard to the brevis.
The Peroneus Tertius
This muscle is distinguished from the longus and brevis by its location and function. The peroneus tertius should be seen more as part of the front of the ankle rather than the lateral side (outside). The peroneus tertius springs more from the front of the fibula to the top of the fifth metatarsal base. Thus, unlike the other peronei, the tertius does not run along the lateral malleolus and, because of this location, is more involved in dorsal flexion(lifting of the foot). Functionally, this contribution is small because of its limited mechanical properties and small size.
How common are peroneal nerve complaints?
Peroneal nerve injuries are probably much more common than is often thought. Exact figures are difficult to determine because this injury is easily missed. This is mainly because peroneal nerve injury rarely occurs in isolation. This means that often the lateral ankle ligaments, for example, are also injured. Various studies show that peroneal nerve injuries range from 11% to 77%, depending on the group studied, with cadaver studies, for example, showing higher rates of injury as opposed to studies in athletes or recreational runners. These varying figures highlight the importance of awareness among healthcare professionals. This often leads to missed or misdiagnosis. Especially in chronic ankle complaints, it appears that peroneal injury is often involved. A consequence is that high-risk groups such as runners, dancers or skaters often do not receive the right advice and treatment for ankle complaints.
How anatomy can affect peroneal tendons
The peroneus longus and brevis both run posteriorly along the lateral malleolus. Space is limited here, which is partly why injuries often occur here. The peroneus longus runs through the cubital tunnel (the brevis does not run in this direction). The shape and space of this cubital tunnel probably influences the occurrence of complaints in this region. Another striking feature is the presence of the os peroneum in this region. The os peroneum is a small bone found in about 20-35% of the population. The function of this small bone is not completely clear. In some cases, the os peroneum seems to provide protection against compression. It makes sliding of the peroneus longus tendon easier without friction. On the other hand, possible disadvantages are also described, it may actually create additional pressure at certain positions of the foot bones, making the tendon more susceptible to irritation or even damage.
On the contrary, the peroneus brevis is vulnerable directly behind the lateral malleolus, where the tendon lies close to the fibula and sometimes gets wedged between the bone and the longus tendon. This can lead to mechanical compression and damage, often in the longitudinal direction of the tendon fibres.
A certain foot and ankle position can also increase the load on the peroneal tendons. For example, a cavovarus position, which is a position with a high instep, creates more compression in the cubital tunnel, which can cause the peroneus longus to be injured more quickly. The position of the foot where only the heel is tilted inwards is called a hindfoot-varus. Mechanically, this puts more pressure on both tendon structures.
Sometimes the problem is more in the available space: a low-running muscle belly of the peroneus brevis can make the tendon sheath narrower, making the tendon more easily trapped. The shape of the fibula can also play a role. A shallow or convex fibular groove offers less protection and makes the tendon more susceptible to displacement (subluxation). When the superior peroneal retinaculum, the ligament that holds the tendons in place, does not provide sufficient support, it can exacerbate instability.
In addition, we see that long-term instability of the ankle is a possible reason for complaints. This puts (too) much demand on the peronei and seems to increase the risk of injury/damage.
Treatment of peroneal nerve injury
The first step in peroneal tendon complaints is usually a conservative approach. Rest and load adjustment are crucial to reduce irritation. Acute tears or severe inflammation may require temporary immobilisation. By this we mean possibly a brace or tape. Physiotherapy focuses mainly on restoring strength, stability and proprioception of the ankle. Here, eccentric exercises have a proven effect in tendinopathies. Load is built up gradually, with clear steps to prevent recurrence.
Surgery for peroneal nerve injury
Surgical intervention may be necessary when physiotherapy does not have the desired effect. In peroneus brevis complaints, this may consist of closing and strengthening longitudinal tears. An operation on the peroneus longus is usually considered when the tendon is torn or severely damaged. During this operation, the tendon is repaired and the channel in which the tendon runs is deepened. Also, the retinaculum that holds the tendons in place, strengthened or made tighter so that the tendons remain stable in place.
Peroneus saltans
A common reason for surgery is peroneus saltans. This involves one or both peroneal tendons on the outside of the ankle clicking over the malleolus. This can happen during movements such as turning the foot outward and is sometimes accompanied by a palpable or audible click. Often, the retinaculum, the band that holds the tendons in place, is damaged. This causes the tendons to repeatedly pop out of their socket, which can cause pain and irritation.
Physio Fitaal in Tilburg Peroneal nerve injury treatment
Complaints of the peroneal nerve can significantly affect your daily activities and sports performance. But with the right approach, recovery is quite possible. Whether you suffer from a sore ankle, a clicking tendon, or long-term problems after an ankle sprain, a correct diagnosis with appropriate treatment makes all the difference.
Our experienced physiotherapists therefore always draw up a personalised treatment plan, tailored to your specific situation and goals. From regular physiotherapy to post-surgery counselling, we are there for you.
Do you have questions about peroneal tendonitis or want to make an appointment? Contact us today. Together, we will make sure you can move pain-free, play sports and enjoy your daily activities again.
